Clinical Trials
and
Case Reports
Clinical Trials
and
Case Reports
Clinical Trials
Clinical Trials
![]()
For decades, electromagnetic therapies have shown clinical effectiveness in treating neurologically-related diseases, wound healing, and bone repair. In this section, we present the clinical trials and pilot studies thus far conducted using Stimpod NMS460 for the treatment of diabetic neuropathies, intractable pain, and migraine.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Long-term, observational study
(India)
Study of the outcome of patients undergoing pulsed radiofrequency for the treatment
of Trigeminal Neuralgia: An observational study.
Neha Sharma, Iqra Nazir Naqash, Zulfiqar Ali, Nadeem Ahmad Khan, Ravouf P Asimi, Imtiyaz A Naqash,
Altaf U Ramzan.
View original article | Download full text PDF
Abstract
Background: Trigeminal neuralgia is chracterised as sudden unilateral severe, stabbing, recurrent episodes of pain in the distribution of one or more branches of
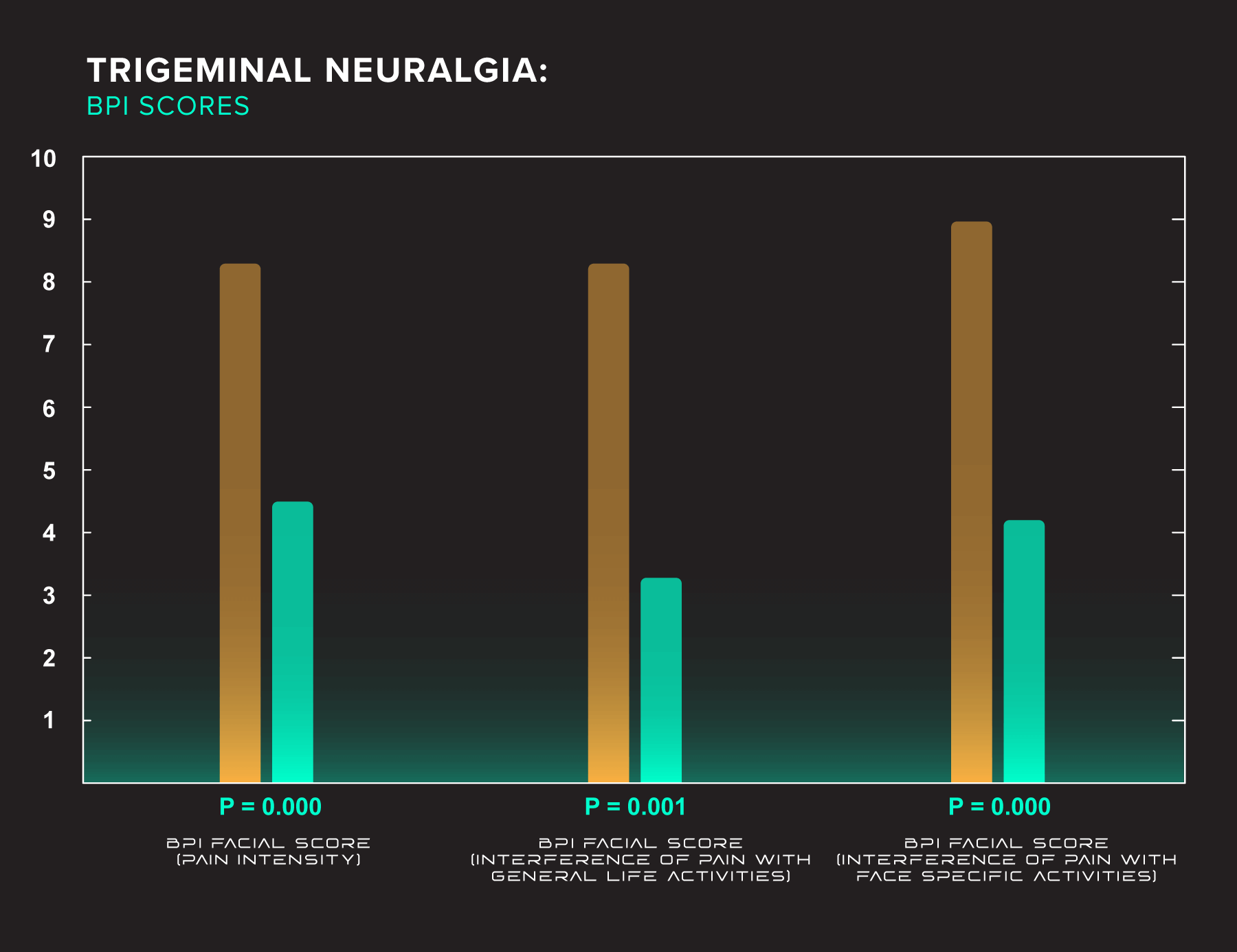
the trigeminal nerve. Pulsed radiofrequency stimulation (PRF) has been recently introduced to alleviate neural, joint pain, and muscle pain. We tried to use PRF for pain relief in trigeminal neuralgia. The primary objective of our study was to observe the effectiveness and safety of pulsed radiofrequency in the patients of trigeminal neuralgia who are refractory to medical management. The secondary objective was to study the effect of pulsed radiofrequency on the duration of pain relief in these patients.
Methodolgy: In this observational study, we enrolled all fresh patients with trigeminal neuralgia attending our pain clinic for the first time and those who had not responded to conservative medical treatment or interventional nerve blocks. All the patients were diagnosed on the basis of signs, symptoms and MRI (CISS sequence). Anatomical landmarks of ophthalarnic nerve, maxillary nerve, mandibular nerve were identified and nerve stimulation was done by placing the probe in the affected nerve division. Each point was stimulated with the radiofrequency probe kept for 10 minutes, giving a current of 10 to 30 milli-amperes with a set frequency of 2 Hertz. A total of 10 settings were given on alternate days. Assessment of pain relief, improvement, or deterioration was done using Barrow Neurological Institute Pain Intensity Score and Brief Pain Inventory facial scale scoring.
Results: There was a significant reduction in pain scores observed on Barrow Neurological Institute (BNI) and Brief Pain Inventory (BPI) pain intensity score (p value of <0.05) before and after pulsed radiofrequency (PRF) application. The duration of pain relief after the application of PRF was up to 180 days in 15 patients, 181-300 days in 8 patients and 300 to 600 days in 7 patients. Only 2 patients had a prolonged pain relief lasting
for 601-720 days. One patient had developed exposure keratitis after 4 sittings of pulsed radiofrequency application at the supraorbital foramen.
Conclusion: PRF offers short term relief in a majority of patients for a period of 18 months to 24 months. However, it was found that the long term effects of PRF may not be seen in patients with TN. PRF may be used as a short term measure for alleviating severe pain of TN till neurolytic
blocks or a definitive surgery is carried out.
Randomized, double-blind, sham-controlled
(India)
Noninvasive neuromodulation of supraorbital and occipital nerves as an adjunct to management of chronic headache
Nazia Tauheed1, Aftab Hussain1, Hira Afzal1, Lubna Zafar2, Hammad Usmani1
1 Department of Anaesthesiology and Critical Care, Jawaharlal Nehru Medical College and Hospital, Aligarh Muslim University, Aligarh, Uttar Pradesh, India
2 Department of Medicine, Jawaharlal Nehru Medical College and Hospital, Aligarh Muslim University, Aligarh, Uttar Pradesh, India
View original article | Download full text PDF
Abstract
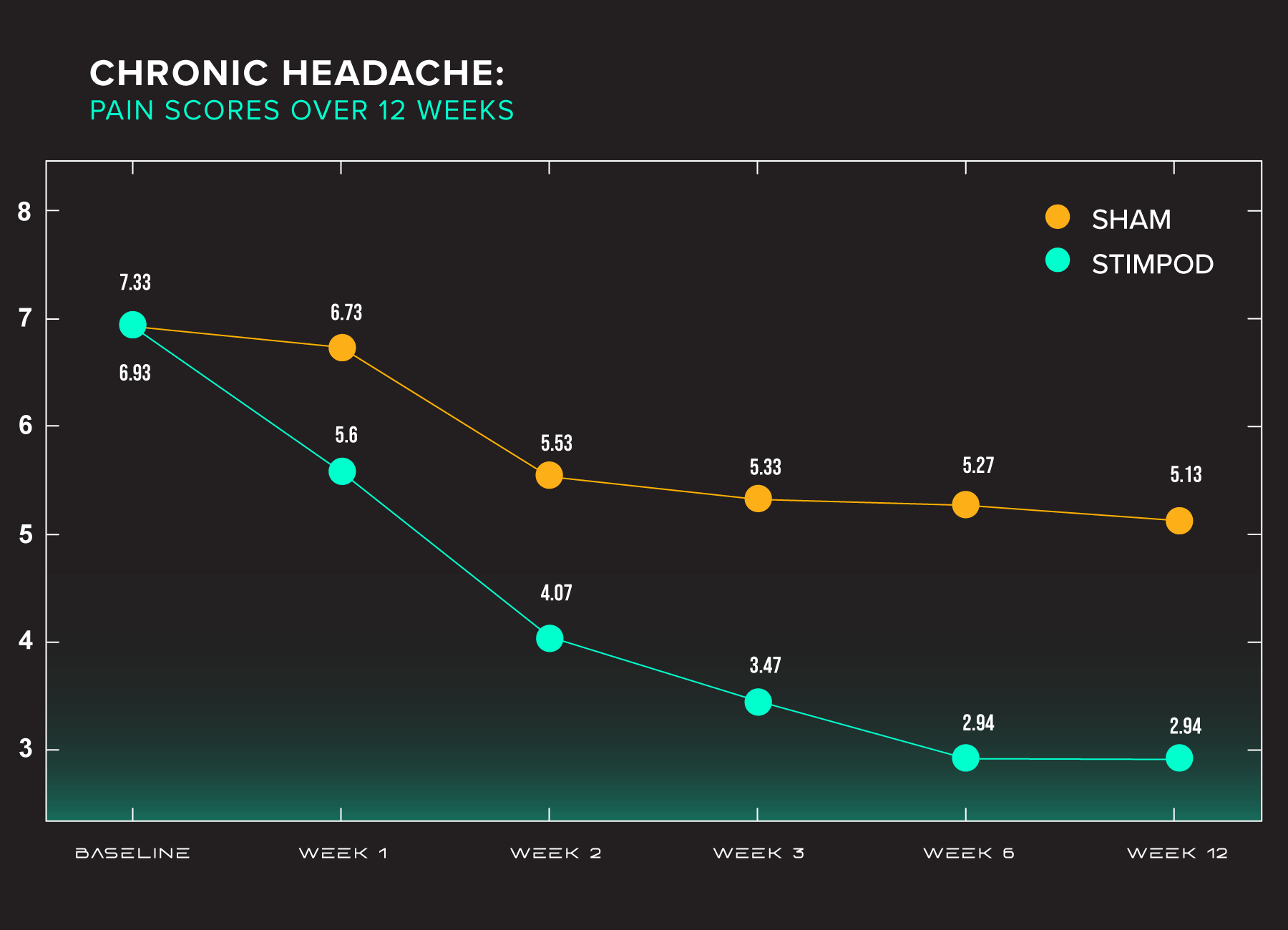
Background: Chronic daily headache (CDH) results in significant distress and a substantial impact on the quality of life. Due to its nature of refractoriness to conservative management, exploring other modalities seems worthwhile. Invasive nerve stimulation, though promising, has seen complication rates in plenty. The goal of the present study was to assess the efficacy of noninvasive neuromodulation of supraorbital and occipital nerves (SON and ON) using hybrid pulsed radiofrequency device (Stimpod NMS460) in patients of CDH.
Methods: Thirty patients suffering from CDH were enrolled in this randomized double‑blind sham‑controlled trial and randomly allocated to two groups of 15 patients each. SON and ON stimulations were given using the device Stimpod NMS460 thrice a week for 3 weeks. Follow‑up visits were scheduled at 6 and 12 weeks of therapy. Pain relief was measured using numerical rating scale score. The overall change in quality of life (measured by Short Form‑12 Health Survey) and associated complications were also noted.
Results: Successful stimulation (50% or greater decrease in pain intensity) was seen in 66.67% patients; inadequate response in 33.3% in the intervention group. The 50% responder rate in sham control group was 13.3%; remaining 86.6% showed an inadequate response. This response remained sustained up to 12 weeks of follow‑up. Similar changes were observed in the quality of life of patients. No adverse effect was documented during the study period.
Conclusion: Noninvasive neuromodulation may serve as a safer and cost‑effective treatment option in CDH refractory to conservative management.
Randomized, single-blind, placebo-controlled
(South Africa)
Can an electrical pulsed radiofrequency device relieve pain and improve function in patients with pedal diabetic neuropathy? A single-blind, randomized placebo-controlled trial.
P. Berger1, S. Landaux2
1University of the Witwatersrand (Faculty of Health Sciences)
2Centre for Diabetes and Endocrinology (CDE) Johannesburg, South Africa
Abstract
Can an electrical pulsed radiofrequency device relieve pain and improve function in patients with pedal diabetic neuropathy? A single-blind randomized placebo-controlled trial.
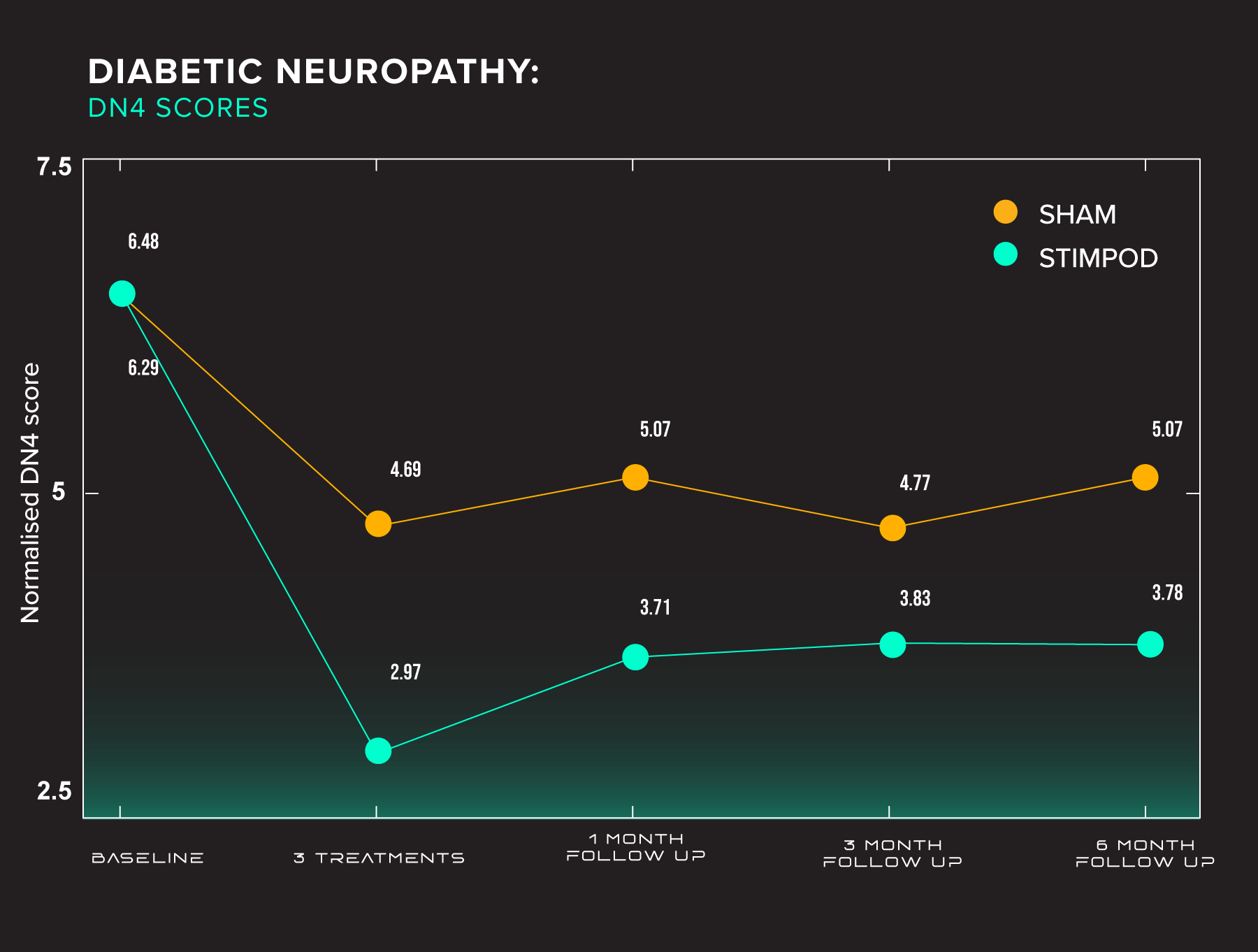
Aim: A randomised single-blind placebo study was conducted on 80 patients with pedal diabetic peripheral neuropathy in 2 cities and their surrounds in South Africa to determine if a pulsed radiofrequency current (PRF) can produce changes in the primary outcome of the DN4 Test and possibly in the BPI-short form.
Method: Patients were selected by their physicians at Centres for Diabetes and randomised into 2 groups – 40 patients each in the groups (A=Active, B =Placebo). Inclusion criteria were pedal Diabetic Peripheral Neuropathy and having a score of 4 or 4+/10 in the DN4 Test. Exclusion criteria: previous experience with the pulsed radiofrequency current and having: peripheral or spinal cord stimulator, pacemaker, metal implants and pregnancy. The DN4 was the primary objective and BPI-SF (secondary) was also tested at baseline, after 3 treatments and 3 follow-ups at 1, 3 and 6 months. Each patient had 3 treatments or a placebo once weekly for 10 mins bilaterally at the sciatic nerve in the popliteal fossa.
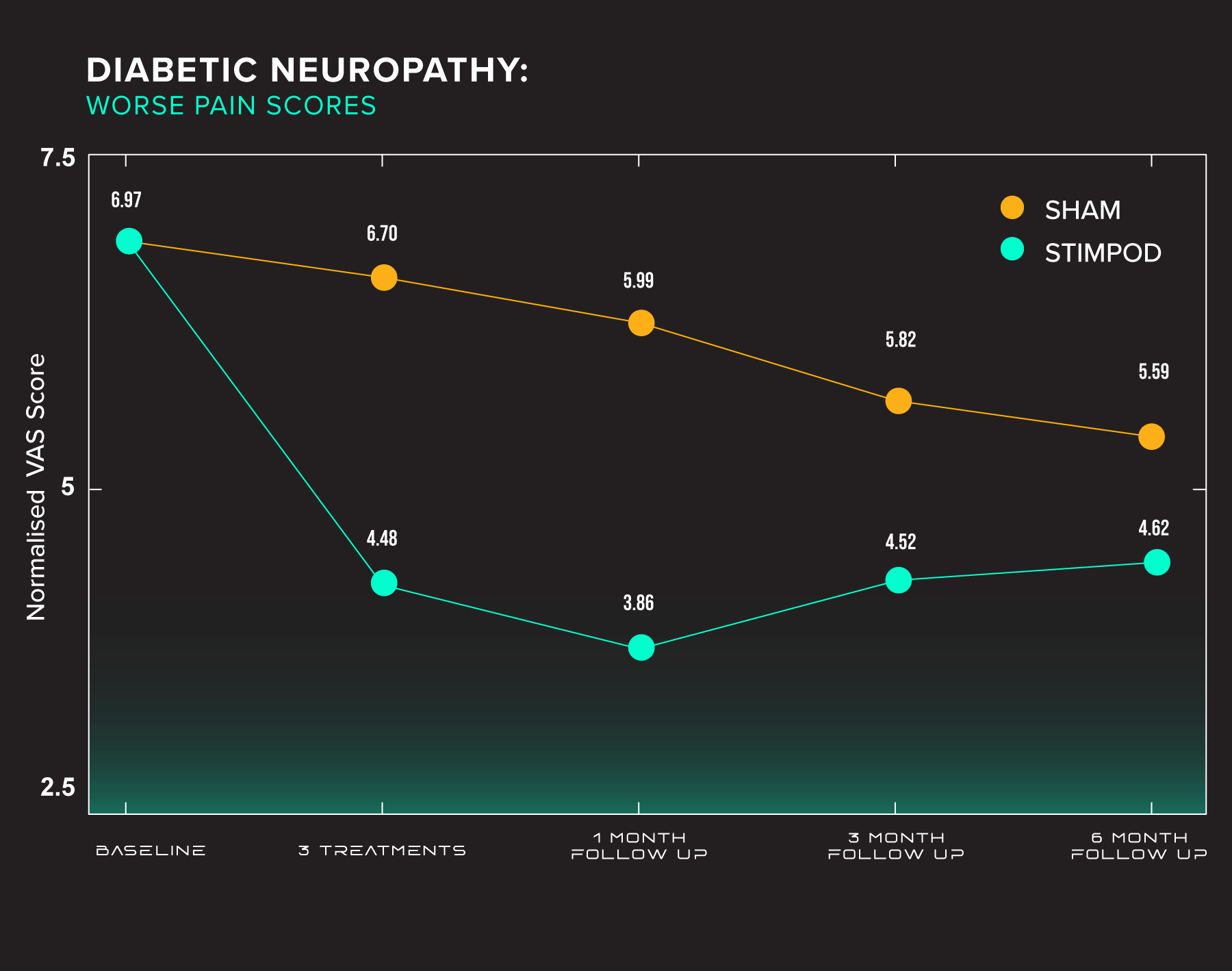
Results: Data were analysed using the SAS version (9.4 statistical program). Results are expressed as mean and standard deviation by groups (A=Active, B=Placebo). There were differences for age and gender in these 2 groups (Age, p=0.030, gender p=0.01) and adjustments were made where applicable. There were also differences evident regardless of age and gender. The DN4 demonstrated that between baseline and 3 treatments there was a reduction in pain and symptoms greater for the A group: p= 0.010 regardless of age and gender. Between baseline and 1 month there was a reduction in pain in both groups, but no significant difference between them p=0.10 but gender and age, nearly significant. There were no differences at 3 and 6 months. In the BPI-SF there were differences between the active and placebo groups in the worst, average and present pain with positive p values some with adjustment for age and gender.
For relations with other people, there was evidence of significant changes some regardless and some adjusted for age and gender and also relations with other people and without analgesics at baseline. There were no differences even after adjustments for age and gender for work and walking ability. None of the BPI-SF variables showed any differences when adjusting for baseline and or analgesics.
Methods
We applied External (transcutaneous) Stimulation to 35 eligible patients complaining of peripheral neuropathic pain. The procedure entailed the application of a 2Hz frequency and amplitude between 1mA and 15mA electrical stimulus (Neurotrace III, predecessor to NMS460) transcutaneously to a targeted area or nerve supplying the area of intractable pain. The duration of stimulation was 5 minutes in each case and pain scores (VAS) were recorded at 0 and 5 minutes.
Conclusion
After three treatments of PRF current, the DN4 Test demonstrates significant improvements in neuropathic pain and symptoms in certain patients with diabetic peripheral neuropathy.
Pain Management Centre, Guy’s & St. Thomas’ Hospitals
(United Kingdom)
External stimulation: simplistic solution to intractable pain
T. Goroszeniuk, S. Kothari
Pain Management Centre, Guy’s & St. Thomas’ Hospitals, London. SE1 7EH. UK
Introduction
Despite adopting a multidisciplinary approach, the management of neuropathic pain not infrequently presents a challenging clinical conundrum. Primary afferent stimulation for the control of chronic pain has been used widely during the last 40 years.
Current locations of access for stimulation include skin in Transcutaneous Electrical Nerve Stimulation (TENS) and acupuncture, peripheral nerve trunks, and primary afferent collaterals in the dorsal columns during Spinal Cord Stimulation (SCS). We have successfully investigated short external low-frequency stimulation either targetted at the site of the maximum pain or deeper afferent sensory nerves in patients with intractable painWe present the preliminary results of our study aimed at symptomatic relief and restoring function in patients with chronic, intractable pain.
Methods
We applied External (transcutaneous) Stimulation to 35 eligible patients complaining of peripheral neuropathic pain. The procedure entailed the application of a 2Hz frequency and amplitude between 1mA and 15mA electrical stimulus (Neurotrace III, predecessor to NMS460) transcutaneously to a targeted area or nerve supplying the area of intractable pain. The duration of stimulation was 5 minutes in each case and pain scores (VAS) were recorded at 0 and 5 minutes.
Results
We noticed a dramatic reduction of the pain VAS. In 19 cases the VAS reduced to 0 at the end of 5 minutes demonstrating a 100% improvement in their pain status. The VAS scores decreased by 90% in four, 63% in another four and 50% in four more patients. The remaining three cases had their VAS score reduce by 25%, 20% and 15% respectively. In four patients with CRPS, vascular changes were observed at end of the procedure.
Conclusion
External stimulation is a noninvasive, simple and effective initial indicator, in patients with neuropathic pain, prior to longer, medium-term percutaneous stimulating catheter trial and subsequent implantation of permanent devices. The external application component allows the procedure to be performed on an outpatient basis and may be considered for diagnostic and repetitive therapeutic procedures. Further investigation is needed to establish a place for this technique in the management of chronic pain.
References:
- Alo K M., Holsheimer J., New trends in neuromodulation for the management of neuropathic pain. Neurosurgery, 2002, 4,690-704.
- Goroszeniuk T., Goroszeniuk D., Short neuromodulation trial in neuropathic pain produces varying duration but reproducible pain relief. Pain in Europe IV. 4th Congress of EFIC, Prague, 2-6.09.2003.
For decades, electromagnetic therapies have shown clinical effectiveness in treating neurologically-related diseases, wound healing, and bone repair. In this section, we present the clinical trials and pilot studies thus far conducted using Stimpod NMS460 for the treatment of diabetic neuropathies, intractable pain, and migraine.
Long-term, observational study
(India)
Study of the outcome of patients undergoing pulsed radiofrequency for the treatment
of Trigeminal Neuralgia: An observational study.
Neha Sharma, Iqra Nazir Naqash, Zulfiqar Ali, Nadeem Ahmad Khan, Ravouf P Asimi, Imtiyaz A Naqash,
Altaf U Ramzan.
View original article | Download full text PDF
Abstract
Background: Trigeminal neuralgia is chracterised as sudden unilateral severe, stabbing, recurrent episodes of pain in the distribution of one or more branches of
the trigeminal nerve. Pulsed radiofrequency stimulation (PRF) has been recently introduced to alleviate neural, joint pain, and muscle pain. We tried to use PRF for pain relief in trigeminal neuralgia. The primary objective of our study was to observe the effectiveness and safety of pulsed radiofrequency in the patients of trigeminal neuralgia who are refractory to medical management. The secondary objective was to study the effect of pulsed radiofrequency on the duration of pain relief in these patients.
Methodolgy: In this observational study, we enrolled all fresh patients with trigeminal neuralgia attending our pain clinic for the first time and those who had not responded to conservative medical treatment or interventional nerve blocks. All the patients were diagnosed on the basis of signs, symptoms and MRI (CISS sequence). Anatomical landmarks of ophthalarnic nerve, maxillary nerve, mandibular nerve were identified and nerve stimulation was done by placing the probe in the affected nerve division. Each point was stimulated with the radiofrequency probe kept for 10 minutes, giving a current of 10 to 30 milli-amperes with a set frequency of 2 Hertz. A total of 10 settings were given on alternate days. Assessment of pain relief, improvement, or deterioration was done using Barrow Neurological Institute Pain Intensity Score and Brief Pain Inventory facial scale scoring.
Results: There was a significant reduction in pain scores observed on Barrow Neurological Institute (BNI) and Brief Pain Inventory (BPI) pain intensity score (p value of <0.05) before and after pulsed radiofrequency (PRF) application. The duration of pain relief after the application of PRF was up to 180 days in 15 patients, 181-300 days in 8 patients and 300 to 600 days in 7 patients. Only 2 patients had a prolonged pain relief lasting
for 601-720 days. One patient had developed exposure keratitis after 4 sittings of pulsed radiofrequency application at the supraorbital foramen.
Conclusion: PRF offers short term relief in a majority of patients for a period of 18 months to 24 months. However, it was found that the long term effects of PRF may not be seen in patients with TN. PRF may be used as a short term measure for alleviating severe pain of TN till neurolytic
blocks or a definitive surgery is carried out.
Randomized, double-blind, sham-controlled
(India)
Noninvasive neuromodulation of supraorbital and occipital nerves as an adjunct to management of chronic headache
Nazia Tauheed1, Aftab Hussain1, Hira Afzal1, Lubna Zafar2, Hammad Usmani1
1 Department of Anaesthesiology and Critical Care, Jawaharlal Nehru Medical College and Hospital, Aligarh Muslim University, Aligarh, Uttar Pradesh, India
2 Department of Medicine, Jawaharlal Nehru Medical College and Hospital, Aligarh Muslim University, Aligarh, Uttar Pradesh, India
View original article | Download full text PDF
Abstract
Background: Chronic daily headache (CDH) results in significant distress and a substantial impact on the quality of life. Due to its nature of refractoriness to conservative management, exploring other modalities seems worthwhile. Invasive nerve stimulation, though promising, has seen complication rates in plenty. The goal of the present study was to assess the efficacy of noninvasive neuromodulation of supraorbital and occipital nerves (SON and ON) using hybrid pulsed radiofrequency device (Stimpod NMS460) in patients of CDH.
Methods: Thirty patients suffering from CDH were enrolled in this randomized double‑blind sham‑controlled trial and randomly allocated to two groups of 15 patients each. SON and ON stimulations were given using the device Stimpod NMS460 thrice a week for 3 weeks. Follow‑up visits were scheduled at 6 and 12 weeks of therapy. Pain relief was measured using numerical rating scale score. The overall change in quality of life (measured by Short Form‑12 Health Survey) and associated complications were also noted.
Results: Successful stimulation (50% or greater decrease in pain intensity) was seen in 66.67% patients; inadequate response in 33.3% in the intervention group. The 50% responder rate in sham control group was 13.3%; remaining 86.6% showed an inadequate response. This response remained sustained up to 12 weeks of follow‑up. Similar changes were observed in the quality of life of patients. No adverse effect was documented during the study period.
Conclusion: Noninvasive neuromodulation may serve as a safer and cost‑effective treatment option in CDH refractory to conservative management.
Randomized, single-blind, placebo-controlled
(South Africa)
Can an electrical pulsed radiofrequency device relieve pain and improve function in patients with pedal diabetic neuropathy? A single-blind, randomized placebo-controlled trial.
P. Berger1, S. Landaux2
1University of the Witwatersrand (Faculty of Health Sciences)
2Centre for Diabetes and Endocrinology (CDE) Johannesburg, South Africa
Abstract
Can an electrical pulsed radiofrequency device relieve pain and improve function in patients with pedal diabetic neuropathy? A single-blind randomized placebo-controlled trial.
Aim: A randomised single-blind placebo study was conducted on 80 patients with pedal diabetic peripheral neuropathy in 2 cities and their surrounds in South Africa to determine if a pulsed radiofrequency current (PRF) can produce changes in the primary outcome of the DN4 Test and possibly in the BPI-short form.
Method: Patients were selected by their physicians at Centres for Diabetes and randomised into 2 groups – 40 patients each in the groups (A=Active, B =Placebo). Inclusion criteria were pedal Diabetic Peripheral Neuropathy and having a score of 4 or 4+/10 in the DN4 Test. Exclusion criteria: previous experience with the pulsed radiofrequency current and having: peripheral or spinal cord stimulator, pacemaker, metal implants and pregnancy. The DN4 was the primary objective and BPI-SF (secondary) was also tested at baseline, after 3 treatments and 3 follow-ups at 1, 3 and 6 months. Each patient had 3 treatments or a placebo once weekly for 10 mins bilaterally at the sciatic nerve in the popliteal fossa.
Results: Data were analysed using the SAS version (9.4 statistical program). Results are expressed as mean and standard deviation by groups (A=Active, B=Placebo). There were differences for age and gender in these 2 groups (Age, p=0.030, gender p=0.01) and adjustments were made where applicable. There were also differences evident regardless of age and gender. The DN4 demonstrated that between baseline and 3 treatments there was a reduction in pain and symptoms greater for the A group: p= 0.010 regardless of age and gender. Between baseline and 1 month there was a reduction in pain in both groups, but no significant difference between them p=0.10 but gender and age, nearly significant. There were no differences at 3 and 6 months. In the BPI-SF there were differences between the active and placebo groups in the worst, average and present pain with positive p values some with adjustment for age and gender.
For relations with other people, there was evidence of significant changes some regardless and some adjusted for age and gender and also relations with other people and without analgesics at baseline. There were no differences even after adjustments for age and gender for work and walking ability. None of the BPI-SF variables showed any differences when adjusting for baseline and or analgesics.
Methods
We applied External (transcutaneous) Stimulation to 35 eligible patients complaining of peripheral neuropathic pain. The procedure entailed the application of a 2Hz frequency and amplitude between 1mA and 15mA electrical stimulus (Neurotrace III, predecessor to NMS460) transcutaneously to a targeted area or nerve supplying the area of intractable pain. The duration of stimulation was 5 minutes in each case and pain scores (VAS) were recorded at 0 and 5 minutes.
Conclusion
After three treatments of PRF current, the DN4 Test demonstrates significant improvements in neuropathic pain and symptoms in certain patients with diabetic peripheral neuropathy.
Pain Management Centre, Guy’s & St. Thomas’ Hospitals
(United Kingdom)
External stimulation: simplistic solution to intractable pain
T. Goroszeniuk, S. Kothari
Pain Management Centre, Guy’s & St. Thomas’ Hospitals, London. SE1 7EH. UK
Introduction
Despite adopting a multidisciplinary approach, the management of neuropathic pain not infrequently presents a challenging clinical conundrum. Primary afferent stimulation for the control of chronic pain has been used widely during the last 40 years.
Current locations of access for stimulation include skin in Transcutaneous Electrical Nerve Stimulation (TENS) and acupuncture, peripheral nerve trunks, and primary afferent collaterals in the dorsal columns during Spinal Cord Stimulation (SCS). We have successfully investigated short external low-frequency stimulation either targetted at the site of the maximum pain or deeper afferent sensory nerves in patients with intractable painWe present the preliminary results of our study aimed at symptomatic relief and restoring function in patients with chronic, intractable pain.
Methods
We applied External (transcutaneous) Stimulation to 35 eligible patients complaining of peripheral neuropathic pain. The procedure entailed the application of a 2Hz frequency and amplitude between 1mA and 15mA electrical stimulus (Neurotrace III, predecessor to NMS460) transcutaneously to a targeted area or nerve supplying the area of intractable pain. The duration of stimulation was 5 minutes in each case and pain scores (VAS) were recorded at 0 and 5 minutes.
Results
We noticed a dramatic reduction of the pain VAS. In 19 cases the VAS reduced to 0 at the end of 5 minutes demonstrating a 100% improvement in their pain status. The VAS scores decreased by 90% in four, 63% in another four and 50% in four more patients. The remaining three cases had their VAS score reduce by 25%, 20% and 15% respectively. In four patients with CRPS, vascular changes were observed at end of the procedure.
Conclusion
External stimulation is a noninvasive, simple and effective initial indicator, in patients with neuropathic pain, prior to longer, medium-term percutaneous stimulating catheter trial and subsequent implantation of permanent devices. The external application component allows the procedure to be performed on an outpatient basis and may be considered for diagnostic and repetitive therapeutic procedures. Further investigation is needed to establish a place for this technique in the management of chronic pain.
References:
- Alo K M., Holsheimer J., New trends in neuromodulation for the management of neuropathic pain. Neurosurgery, 2002, 4,690-704.
- Goroszeniuk T., Goroszeniuk D., Short neuromodulation trial in neuropathic pain produces varying duration but reproducible pain relief. Pain in Europe IV. 4th Congress of EFIC, Prague, 2-6.09.2003.
Case Reports
![]()
Case Reports
The reports listed in this section has shown such dramatic impact that practitioners using the Stimpod NMS460 felt compelled to share the results with us.
A Case Report on a Patient With Unrecovered Bell’s Palsy of 2 Years Duration Treated With Non-Interventional Pulsed Radio Frequency Electrical Current
Phyllis Berger
Adjunct Professor – School of Therapeutic Sciences; Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
View original article | Download full text PDF
Abstract
A Case Report on a Patient With Noninvasive pulsed radiofrequency for trigeminal neuralgia: Off the beaten path – Case series
Sukanya Mitra, Prateek Upadhyay, Jasveer Singh, Prashant Ahlawat
View original article | Download full text PDF
Abstract
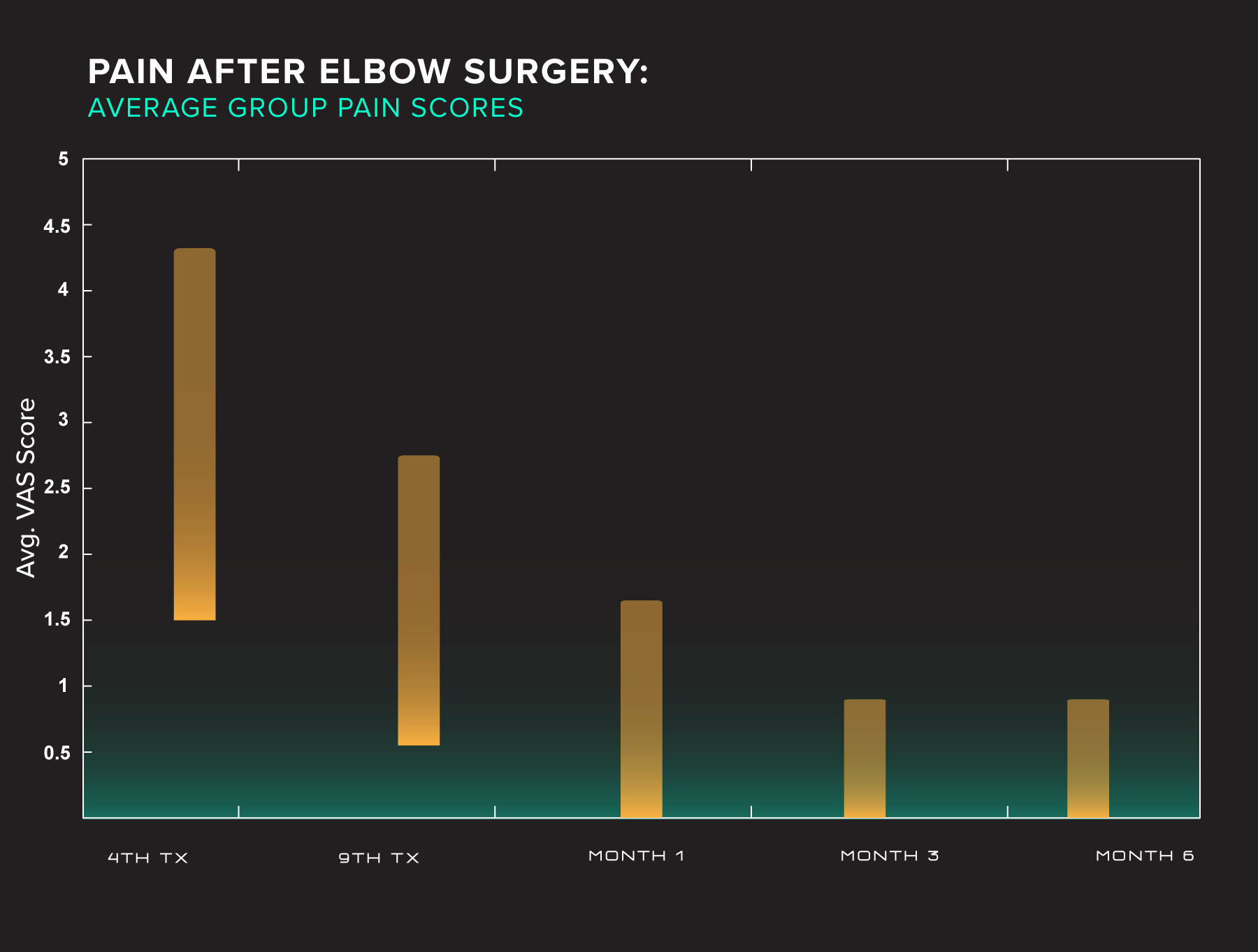
Report on a case series investigating a neurostimulation device for the treatment of pain and improvement of mobility and function following elbow surgery
P. Berger, J. Jacks
Pain Management Physiotherapy, Rochester Place, 173 Rivonia Road, Morningside, Johannesburg, South Africa
View original article | Download full text PDF
Introduction
Patients undergoing epicondylitis surgery whether medial or lateral have had chronic elbow pain for a prolonged period often of many months to a year in some cases that has been unresponsive to conservative measures.
Although epicondylitis is a common condition in the arm due to physical overload, the prevalence of definitive lateral epicondylitis was 1.3% and that of medial epicondylitis was 0.4% according to a study in Finland (between 2000 and 2001). The prevalence did not differ between men and women and was highest in subjects aged 45–54 years [1,5]. Prior to surgery these patients have usually had non-surgical treatment and conservative care that includes decreased activity, ice, non-steroidal anti-inflammatory medications, muscle strengthening [2] and these modalities usually help most people. Recalcitrant cases may require cortisone injections that demonstrate the best conservative treatment for lateral epicondylitis [3] but provides only short-term benefits in medial epicondylitis [4]. Lateral epicondylitis, also known as “tennis elbow,” is an overuse syndrome of the common extensor tendon, predominantly affecting the extensor carpi radialis brevis. Patients complain of poorly defined pain located over the lateral elbow that is typically exacerbated by activities requiring wrist extension and/or wrist supination against resistance. There will often be pain in the morning as well as after any period of time that the elbow has been held in a flexed position [5]. Medial epicondylitis is a clinical entity characterized by pain in the medial aspect of the elbow and dysfunction induced by degenerative changes in the origin of the flexor–pronator muscle mass.The accumulated pathological evidence suggests that the process is associated with fibrillary degeneration of collagen and angiofibroblastic hyperplasia at the origin of the flexor pronator muscle mass, microfragmentation or tears of the tendon, accumulation of vascular granulation tissue and tendinous necrosis, all of which are also accompanied by a secondary inflammatory reaction [6]. Non-operative treatment has been deemed highly successful,yet the few prospective reports available suggest that symptoms frequently persist or recur. Operative treatment is indicated for debilitating pain that is diagnosed after the exclusion of other pathologic causes for pain and that persists in spite of a well-managed non-operative regimen spanning a minimum of 6 months. The surgical technique involves excision of the pathologic portion of the tendon, repair of the resulting defect, and reattachment of the origin to the lateral or medial epicondyle.
Surgical treatment results in a high degree of subjective relief, although objective strength deficits may persist [7]. During the last decade, increased attention has been paid to persistent pain complaints after almost any surgical operation with reported incidences ranging between 5% and 50% [8]. The International Association for the Study of Pain defines post-surgical pain as persistent pain after surgery of greater than three months duration[9]. Persistent post-surgical pain syndromes (PPSP) have been considered neuropathic [8] and a strong association is reported between PPSP and sensory abnormalities [10]; however, there is evidence that mechanisms other than nerve injury such as inflammation, central sensitization or a combination of these may play a role. It is important to elucidate whether persistent pain is due to surgical injury of the nerves, ongoing inflammatory processes,injury to the somatic or visceral structures or other causes [11]. Most of those patients that elected to have the surgery for the elbow in these case reports had chronic pain before surgery with or without neuropathic symptoms. It was thought that treating the acute post-operative pain aggressively early by blocking pain,improving wound healing and improving strength may have some impact on post-surgical pain.
Methods
Seven patients who had elbow surgery either for golfers or tennis elbow were sent for neurostimulation within a day post-surgery. The University of the Witwatersrand Human Ethics Committee approval was received for the study. An information and consent form was presented to patients and duly signed.
The treatment protocol was divided into two sections.
The first three treatments with non-invasive pulsed radio frequency:
- 20 min in total
- brachial plexus region for 10 min superior to the clavicle
- brachial plexus region for 10 min inferior to the clavicle
This treatment was given on alternate days over 1 week before the splint was removed and the aim was to reduce pain immediately and to have a possible influence on post-operative pain syndromes that may occur, to prime the nerve supply to the elbow to increase mobility and to improve muscle strength (this could be visualized by fasciculation of the muscles under the splint) to enable better function after the splint was removed.
Once the splint was removed all measures and evaluations were taken before the second section of treatment was implemented.
Results
In the patient study group there were four females and three males and the ages ranged from 38 to 60 years. Only one patient had a golfers elbow repair the remainder had a tennis elbow repair. Five patients recovered well and two patients had to have the surgery redone due in the first patient to a complication within the arm due to a previous knife wound and a more extensive approach being required than as in the initial surgery and in the other patient re-operation was required after a fall that had occurred during the recovery period damaging the original site of the surgery.
There was significant pain post-surgery but the movements of flexion and extension were already quite advanced immediately after the splint was removed and this may have been expedited by the electrical stimulation. There were only two movements such as making a fist and washing the face that were evaluated on the fourth treatment as all others were not attainable and there were 12 movements that were attainable and evaluated from the sixth to ninth treatment.
Patient 107 had a good range of movement of flexion and patient 102 had a good range of extension before the 4th treatment.
On the last treatment, pain levels were greatly reduced except for the patient that had to be re-operated. Range of movements and activities were achieved or almost full.
Electrical current and acupuncture treatment for a paediatric patient with recurring long thoracic nerve paralysis
By Prof. Phyllis Berger
View original article | Download full text PDF
Abstract
A female paediatric patient aged 9 years presented with right long thoracic nerve palsy for the second time. The first injury that occurred in 2011 was due to a fall and although the patient had a paralysis of the serratus anterior muscle and was unable to elevate the arm, with rehabilitation and conventional physiotherapy, she recovered completely according to the nerve conduction test that was conducted six months post-recovery.
The second injury to the long thoracic nerve was due to a ballet movement that occurred in 2012. Besides the nerve palsy that reoccurred, there was also a complication of severe pain and evidence of a complex regional pain syndrome (CRPS). The second injury was limited by the inability to participate in rehabilitation exercises and physiotherapy due to pain and hyperaesthesia in the distribution of C5 and C6 dermatome both in the trapezius and shoulder region. The third nerve conduction test deteriorated to those recorded after the first nerve conduction test.
A different physiotherapy approach was then applied – initially to reduce pain and decrease hyperaesthesia and then to attempt to increase nerve conduction by the inclusion of an electrical device that simultaneously delivers both a low and a high-frequency current. This treatment was combined with various pain resolving tactics including acupuncture, individual sub-liminal, low and high-frequency electrical currents. Several interventions were applied to tailor the treatment to the patient to achieve maximal improvement in pain and mobility. It is therefore difficult to attribute improvement to one particular modality or even natural resolution of the condition however previous clinical application and experience of activating nerve conduction with the combination current in other conditions implied that improvement could be expected. This particular electrical current is a combination of a low frequency and a magnetic field.
The condition resolved completely with full movement and no pain after 13 treatments over two months – it was evident that the combination of treatment had an effect on expediting the healing in the nerve. The patient was able to resume all her normal activities including gymnastics and ballet.
Feasibility of a promising pulsed electrostimulator for rapid motor recovery of foot drop
Yu-Cheng Changa, Yuan-Ping Chao, Shin-Tsu Chang
View full text article: Pubmed Central | Heliyon
Abstract
Foot drop still occurs in clinical practice, including in our case. Treatments for foot drop vary based on its etiology and severity of symptoms. Hence, in intractable foot drop cases, an invasive surgical intervention is needed. Here, we introduce a special noninvasive technique to treat our patient’s foot drop. In this approach, we applied STIMPOD NMS460 neuromuscular stimulator device (STIMPOD NMS460), which is a low-frequency (10 Hz or less) transcutaneous electrical nerve stimulation (TENS) device with a pulsed radiofrequency (PRF) component. We are eager to know how effective the device is in treating foot drop, and we compared it with two kinds of surgical interventions.
Materials and Method
The device settings are 5 Hz in frequency and 30mA in current amplitude. The device was applied on her left side at the L4 and L5 regions and at the fibular head. Each therapy session consists of individual 15-min treatments on these two body areas, and it only takes a total of 30 minutes. We recorded the change in ankle dorsiflexion degrees and muscle strength of our patient.
Results and Conclusion
To our surprise, our patient’s actual treatment status through STIMPOD NMS460 showed more effective recovery and no specific side effects than surgical interventions in similar conditions. Besides, after a three-month intervention, her affected ankle dorsiflexion recovered to almost her usual status. The reason why this device has such an effect may be that it has the benefits of TENS and PRF. Besides, some studies have revealed the nerve-repair effect of TENS and PRF. In conclusion, we believe that this device is fairly promising and may be qualified to be used in other patients with foot drop.
Citation and links:
Chang YC, Chao YP, Chang ST. Feasibility of a promising pulsed electrostimulator for rapid motor recovery of foot drop. Heliyon. 2024 Feb 1;10(3):e25176. doi: 10.1016/j.heliyon.2024.e25176. PMID: 38327404; PMCID: PMC10847864.
Pubmed Central: Feasibility of a promising pulsed electrostimulator for rapid motor recovery of foot drop
Heliyon: Feasibility of a promising pulsed electrostimulator for rapid motor recovery of foot drop
The reports listed in this section has shown such dramatic impact that practitioners using the Stimpod NMS460 felt compelled to share the results with us.
A Case Report on a Patient With Unrecovered Bell’s Palsy of 2 Years Duration Treated With Non-Interventional Pulsed Radio Frequency Electrical Current
Phyllis Berger
Adjunct Professor – School of Therapeutic Sciences; Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
View original article | Download full text PDF
Abstract
A Case Report on a Patient With Noninvasive pulsed radiofrequency for trigeminal neuralgia: Off the beaten path – Case series
Sukanya Mitra, Prateek Upadhyay, Jasveer Singh, Prashant Ahlawat
View original article | Download full text PDF
Abstract
Report on a case series investigating a neurostimulation device for the treatment of pain and improvement of mobility and function following elbow surgery
P. Berger, J. Jacks
Pain Management Physiotherapy, Rochester Place, 173 Rivonia Road, Morningside, Johannesburg, South Africa
View original article | Download full text PDF
Introduction
Patients undergoing epicondylitis surgery whether medial or lateral have had chronic elbow pain for a prolonged period often of many months to a year in some cases that has been unresponsive to conservative measures.
Although epicondylitis is a common condition in the arm due to physical overload, the prevalence of definitive lateral epicondylitis was 1.3% and that of medial epicondylitis was 0.4% according to a study in Finland (between 2000 and 2001). The prevalence did not differ between men and women and was highest in subjects aged 45–54 years [1,5]. Prior to surgery these patients have usually had non-surgical treatment and conservative care that includes decreased activity, ice, non-steroidal anti-inflammatory medications, muscle strengthening [2] and these modalities usually help most people. Recalcitrant cases may require cortisone injections that demonstrate the best conservative treatment for lateral epicondylitis [3] but provides only short-term benefits in medial epicondylitis [4]. Lateral epicondylitis, also known as “tennis elbow,” is an overuse syndrome of the common extensor tendon, predominantly affecting the extensor carpi radialis brevis. Patients complain of poorly defined pain located over the lateral elbow that is typically exacerbated by activities requiring wrist extension and/or wrist supination against resistance. There will often be pain in the morning as well as after any period of time that the elbow has been held in a flexed position [5]. Medial epicondylitis is a clinical entity characterized by pain in the medial aspect of the elbow and dysfunction induced by degenerative changes in the origin of the flexor–pronator muscle mass.The accumulated pathological evidence suggests that the process is associated with fibrillary degeneration of collagen and angiofibroblastic hyperplasia at the origin of the flexor pronator muscle mass, microfragmentation or tears of the tendon, accumulation of vascular granulation tissue and tendinous necrosis, all of which are also accompanied by a secondary inflammatory reaction [6]. Non-operative treatment has been deemed highly successful,yet the few prospective reports available suggest that symptoms frequently persist or recur. Operative treatment is indicated for debilitating pain that is diagnosed after the exclusion of other pathologic causes for pain and that persists in spite of a well-managed non-operative regimen spanning a minimum of 6 months. The surgical technique involves excision of the pathologic portion of the tendon, repair of the resulting defect, and reattachment of the origin to the lateral or medial epicondyle.
Surgical treatment results in a high degree of subjective relief, although objective strength deficits may persist [7]. During the last decade, increased attention has been paid to persistent pain complaints after almost any surgical operation with reported incidences ranging between 5% and 50% [8]. The International Association for the Study of Pain defines post-surgical pain as persistent pain after surgery of greater than three months duration[9]. Persistent post-surgical pain syndromes (PPSP) have been considered neuropathic [8] and a strong association is reported between PPSP and sensory abnormalities [10]; however, there is evidence that mechanisms other than nerve injury such as inflammation, central sensitization or a combination of these may play a role. It is important to elucidate whether persistent pain is due to surgical injury of the nerves, ongoing inflammatory processes,injury to the somatic or visceral structures or other causes [11]. Most of those patients that elected to have the surgery for the elbow in these case reports had chronic pain before surgery with or without neuropathic symptoms. It was thought that treating the acute post-operative pain aggressively early by blocking pain,improving wound healing and improving strength may have some impact on post-surgical pain.
Methods
Seven patients who had elbow surgery either for golfers or tennis elbow were sent for neurostimulation within a day post-surgery. The University of the Witwatersrand Human Ethics Committee approval was received for the study. An information and consent form was presented to patients and duly signed.
The treatment protocol was divided into two sections.
The first three treatments with non-invasive pulsed radio frequency:
- 20 min in total
- brachial plexus region for 10 min superior to the clavicle
- brachial plexus region for 10 min inferior to the clavicle
This treatment was given on alternate days over 1 week before the splint was removed and the aim was to reduce pain immediately and to have a possible influence on post-operative pain syndromes that may occur, to prime the nerve supply to the elbow to increase mobility and to improve muscle strength (this could be visualized by fasciculation of the muscles under the splint) to enable better function after the splint was removed.
Once the splint was removed all measures and evaluations were taken before the second section of treatment was implemented.
Results
In the patient study group there were four females and three males and the ages ranged from 38 to 60 years. Only one patient had a golfers elbow repair the remainder had a tennis elbow repair. Five patients recovered well and two patients had to have the surgery redone due in the first patient to a complication within the arm due to a previous knife wound and a more extensive approach being required than as in the initial surgery and in the other patient re-operation was required after a fall that had occurred during the recovery period damaging the original site of the surgery.
There was significant pain post-surgery but the movements of flexion and extension were already quite advanced immediately after the splint was removed and this may have been expedited by the electrical stimulation. There were only two movements such as making a fist and washing the face that were evaluated on the fourth treatment as all others were not attainable and there were 12 movements that were attainable and evaluated from the sixth to ninth treatment.
Patient 107 had a good range of movement of flexion and patient 102 had a good range of extension before the 4th treatment.
On the last treatment, pain levels were greatly reduced except for the patient that had to be re-operated. Range of movements and activities were achieved or almost full.
Electrical current and acupuncture treatment for a paediatric patient with recurring long thoracic nerve paralysis
By Prof. Phyllis Berger
View original article | Download full text PDF
Abstract
A female paediatric patient aged 9 years presented with right long thoracic nerve palsy for the second time. The first injury that occurred in 2011 was due to a fall and although the patient had a paralysis of the serratus anterior muscle and was unable to elevate the arm, with rehabilitation and conventional physiotherapy, she recovered completely according to the nerve conduction test that was conducted six months post-recovery.
The second injury to the long thoracic nerve was due to a ballet movement that occurred in 2012. Besides the nerve palsy that reoccurred, there was also a complication of severe pain and evidence of a complex regional pain syndrome (CRPS). The second injury was limited by the inability to participate in rehabilitation exercises and physiotherapy due to pain and hyperaesthesia in the distribution of C5 and C6 dermatome both in the trapezius and shoulder region. The third nerve conduction test deteriorated to those recorded after the first nerve conduction test.
A different physiotherapy approach was then applied – initially to reduce pain and decrease hyperaesthesia and then to attempt to increase nerve conduction by the inclusion of an electrical device that simultaneously delivers both a low and a high-frequency current. This treatment was combined with various pain resolving tactics including acupuncture, individual sub-liminal, low and high-frequency electrical currents. Several interventions were applied to tailor the treatment to the patient to achieve maximal improvement in pain and mobility. It is therefore difficult to attribute improvement to one particular modality or even natural resolution of the condition however previous clinical application and experience of activating nerve conduction with the combination current in other conditions implied that improvement could be expected. This particular electrical current is a combination of a low frequency and a magnetic field.
The condition resolved completely with full movement and no pain after 13 treatments over two months – it was evident that the combination of treatment had an effect on expediting the healing in the nerve. The patient was able to resume all her normal activities including gymnastics and ballet.
Feasibility of a promising pulsed electrostimulator for rapid motor recovery of foot drop
Yu-Cheng Changa, Yuan-Ping Chao, Shin-Tsu Chang
View full text article: Pubmed Central | Heliyon
Abstract
Foot drop still occurs in clinical practice, including in our case. Treatments for foot drop vary based on its etiology and severity of symptoms. Hence, in intractable foot drop cases, an invasive surgical intervention is needed. Here, we introduce a special noninvasive technique to treat our patient’s foot drop. In this approach, we applied STIMPOD NMS460 neuromuscular stimulator device (STIMPOD NMS460), which is a low-frequency (10 Hz or less) transcutaneous electrical nerve stimulation (TENS) device with a pulsed radiofrequency (PRF) component. We are eager to know how effective the device is in treating foot drop, and we compared it with two kinds of surgical interventions.
Materials and Method
The device settings are 5 Hz in frequency and 30mA in current amplitude. The device was applied on her left side at the L4 and L5 regions and at the fibular head. Each therapy session consists of individual 15-min treatments on these two body areas, and it only takes a total of 30 minutes. We recorded the change in ankle dorsiflexion degrees and muscle strength of our patient.
Results and Conclusion
To our surprise, our patient’s actual treatment status through STIMPOD NMS460 showed more effective recovery and no specific side effects than surgical interventions in similar conditions. Besides, after a three-month intervention, her affected ankle dorsiflexion recovered to almost her usual status. The reason why this device has such an effect may be that it has the benefits of TENS and PRF. Besides, some studies have revealed the nerve-repair effect of TENS and PRF. In conclusion, we believe that this device is fairly promising and may be qualified to be used in other patients with foot drop.
Citation and links:
Chang YC, Chao YP, Chang ST. Feasibility of a promising pulsed electrostimulator for rapid motor recovery of foot drop. Heliyon. 2024 Feb 1;10(3):e25176. doi: 10.1016/j.heliyon.2024.e25176. PMID: 38327404; PMCID: PMC10847864.
Pubmed Central: Feasibility of a promising pulsed electrostimulator for rapid motor recovery of foot drop
Heliyon: Feasibility of a promising pulsed electrostimulator for rapid motor recovery of foot drop